TL;DR:
- AI-powered patient communication now uses large language models, retrieval-augmented generation, and triage logic to manage inquiries autonomously. Clinics must ensure HIPAA compliance, verify specialty-specific accuracy, and implement automated quality monitoring for effective deployment. Successful strategies involve clear inquiry scope, structured escalation, integration with existing systems, and rigorous ongoing performance evaluation.
AI-powered patient communication is defined as the use of intelligent systems to receive, classify, and respond to patient questions, scheduling requests, and clinical concerns without requiring a staff member to pick up the phone. How AI handles clinic inquiries has moved well beyond simple chatbots. Systems deployed at Vanderbilt Health and Penn Medicine now use large language models, retrieval-augmented generation, and triage logic to manage the full inquiry lifecycle. For healthcare administrators, understanding this architecture is not optional. It is the foundation for any serious decision about deploying AI in a clinical setting.
How AI handles clinic inquiries: the core workflow
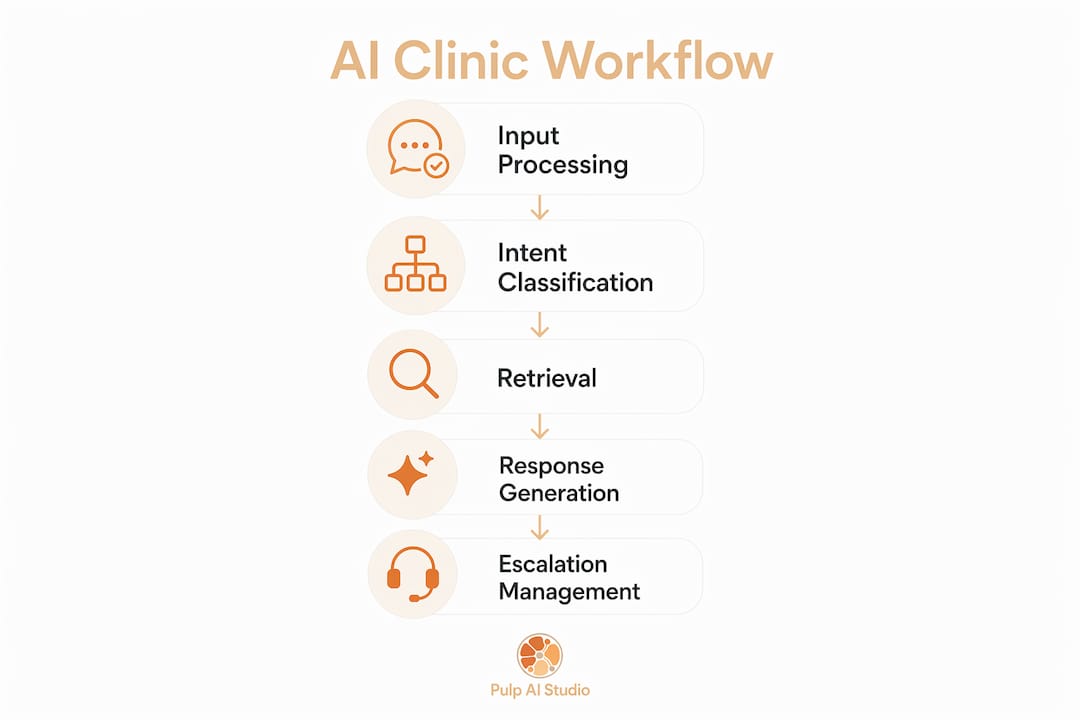
AI inquiry handling is not simply natural language generation. It routes patient requests through triage logic that mimics clinical workflows, separating routine requests from those requiring a licensed clinician. The process starts the moment a patient submits a question through a portal, calls a front desk line, or sends a text. The AI classifies the intent, pulls relevant institutional knowledge, and either resolves the inquiry or escalates it.

Here is the way to think about it: the AI is the intake coordinator who never sleeps. It reads the question, decides whether it can handle it, and either answers or hands it off. What makes clinic-specific AI different from a generic chatbot is the integration of institutional knowledge and clinical guardrails. A generic chatbot answers from general training data. A clinic-specific system answers from your protocols, your formulary, your scheduling rules.
Vanderbilt Health launched its AI assistant on April 1, 2026. When a patient selects “medical question” in the portal, the assistant asks clarifying follow-ups before drafting a message for care team review. The patient gets a clearer, more complete message sent to their provider. The care team receives a structured, actionable question instead of a vague complaint. That is the operational payoff administrators should focus on.
What technologies power AI medical inquiry processing?
The architecture behind modern AI inquiry systems has four primary components: large language models (LLMs), retrieval-augmented generation (RAG), intent classification, and EHR integration.
LLMs are the reasoning engine. Models like those from OpenAI process natural language and generate contextually appropriate responses. They understand that “my knee has been swollen for a week” is different from “I need to reschedule my appointment.” The model reads the patient’s words and determines what type of response is needed.
RAG is what separates a clinic-grade system from a consumer chatbot. Vanderbilt’s assistant uses retrieval-augmented generation to pull institution-specific triage protocols and nursing care-routing instructions before generating a response. The model does not guess. It retrieves the correct clinical context and builds its answer on top of it.
Intent classification determines what the patient actually wants. A patient message might contain a symptom description, a scheduling request, and a billing question all in one paragraph. The AI parses these into separate intents and routes each one appropriately.
EHR integration closes the loop. The K Health and Penn Medicine collaboration, announced in May 2026, deploys AI clinical agents that conduct personalized patient intake and pre-populate EHR drafts. The clinician walks into the room with a structured intake note already generated. That is time recaptured from administrative work and returned to direct patient care.
Here is a breakdown of what each technology layer handles:
- LLMs: Generate natural language responses and interpret patient intent from unstructured text
- RAG: Pull institution-specific protocols, formularies, and routing rules to ground responses in clinical reality
- Intent classification: Sort incoming inquiries by type (clinical, scheduling, billing, urgent) and route accordingly
- EHR integration: Pre-populate intake notes, flag relevant history, and reduce manual data entry for clinical staff
- Triage protocols: Define the boundary between what the AI resolves and what escalates to a human clinician
Pro Tip: When evaluating AI vendors, ask specifically whether their system uses RAG or relies solely on base model training. A RAG-enabled system can be updated with your latest protocols without retraining the entire model. That distinction matters operationally.
How accurate is AI when answering medical questions?
Accuracy is where administrators need to be clear-eyed. LLM-generated health query responses achieve roughly 76.2% overall accuracy, with error rates exceeding 20%. That means roughly one in five AI-generated medical responses contains a clinically meaningful mistake. That number should not be dismissed as acceptable variance.
The Penn State study also found that accuracy varies significantly by medical specialty. Some domains perform well above the average; others fall below it. The implication is that a single accuracy figure does not tell you how the system will perform in your specific clinical context. A dermatology practice and a cardiology clinic will see different error profiles from the same AI system.
| Accuracy factor | What it means for your clinic |
|---|---|
| Overall accuracy ~76% | Roughly 1 in 4 responses requires human correction or review |
| Specialty variation | Test AI accuracy specifically in your clinical domain before deployment |
| Prompt specificity | Queries with 60–250 characters and specific phrasing produce more accurate responses |
| Training data quality | Systems trained on real-world clinical interactions outperform those trained on general text |
| Automated evaluation | Scalable quality checks aligned with clinician ratings reduce manual review burden |
Prompt specificity matters more than most administrators realize. The Penn State research found that specific phrasing and character count in the 60 to 250 character range improved accuracy meaningfully. This means the way your intake forms and portal prompts are written directly affects how accurately the AI responds. Poorly worded patient prompts produce poorly structured AI responses.
Quality assurance at scale is now achievable without manual expert review for every interaction. An npj Digital Medicine study tested 28 AI systems across 100 hospitalized patient cases and found that automated evaluation metrics align closely with human expert ratings. Clinics can now run automated pipelines that measure completeness, evidence use, and medical knowledge without a physician reviewing every response. That is what makes ongoing monitoring operationally realistic.
Pro Tip: Do not deploy AI for clinical inquiries without defining a specialty-specific accuracy threshold. Set a minimum acceptable accuracy rate for your domain, run a pilot with 200 to 300 real patient inquiries, and measure against that threshold before full rollout.
What compliance requirements apply to AI in clinic inquiry handling?
HIPAA compliance is non-negotiable when AI systems touch protected health information (PHI). AI voice agents and chatbots that process patient data are classified as HIPAA business associates, which means your clinic must have a signed Business Associate Agreement (BAA) with every AI vendor before a single patient message is processed. No BAA means no deployment. That is the starting point.
Beyond the BAA, the technical safeguards required under HIPAA apply in full:
- Encryption: All PHI must be encrypted in transit and at rest. Confirm the vendor uses TLS 1.2 or higher for data in transit and AES-256 for stored data.
- Access controls: Role-based access must limit who can view AI interaction logs. Not every staff member needs access to every patient conversation.
- Audit logs: Every AI interaction involving PHI must be logged with timestamps, user identifiers, and action records. These logs are what you produce during a HIPAA audit.
- Breach notification procedures: Your AI vendor must have documented breach response protocols and must notify you within the timeframes HIPAA requires.
- State call recording laws: If your AI system records voice calls, state consent laws apply. Some states require two-party consent. This is a separate legal layer on top of HIPAA that many administrators overlook.
Vendor vetting is where compliance either holds or breaks down. Ask every AI vendor for their most recent HIPAA risk assessment, their BAA template, and documentation of their encryption standards. A vendor who cannot produce these documents quickly is not a vendor you want handling your patient data. For a deeper look at what HIPAA-compliant agent communication requires in practice, the technical and legal considerations go well beyond the BAA itself.
The practical advice here is to treat AI vendor selection as a compliance decision first and a technology decision second. The best AI system in the world creates liability if it is not properly configured for PHI handling.
What deployment strategies actually work in clinical settings?
The deployment model that works is a two-layer architecture. Layer one handles inquiry capture and clarification. Layer two manages escalation to human clinicians for anything outside defined guardrails. This is not a theoretical framework. It is what Vanderbilt and Penn Medicine have built into their live systems.
Here is how to structure a practical rollout:
-
Define the inquiry scope. Decide which inquiry types the AI will handle autonomously: appointment scheduling, prescription refill requests, billing questions, and general information. Define which types always escalate: urgent symptoms, medication dosage questions, and anything requiring clinical judgment.
-
Map your escalation triggers. Build explicit rules for when the AI hands off to a human. These triggers should be based on your triage protocols, not the AI vendor’s defaults. Vanderbilt’s system uses institutional triage logic to determine when a question exceeds the AI’s safe operating scope.
-
Integrate with your existing digital front door. Penn Medicine’s AI clinical agents connect directly to the patient portal and EHR. The AI does not operate as a standalone tool. It feeds structured data into the systems your clinical staff already use. This is what makes the patient intake workflow efficient rather than duplicative.
-
Set up automated monitoring from day one. Use automated evaluation pipelines to measure response completeness and accuracy on an ongoing basis. The npj Digital Medicine research confirms that automated rankings match clinician judgments when anchored to clinician-authored reference answers. You do not need a physician reviewing every AI response. You need a well-designed automated scoring system.
-
Measure operational outcomes monthly. Track hold time reduction, staff inquiry volume, after-hours inquiry capture rate, and patient satisfaction scores. These are the numbers that justify continued investment and identify where the system needs refinement.
The operational benefits are real. Clinics using AI for routine inquiry automation report reduced hold times, lower staff burnout from repetitive call handling, and improved patient engagement scores. The AI employee handles the volume. Your clinical staff handles the complexity. That division of labor is what makes the model work.
Key takeaways
AI inquiry handling in clinics works when it combines institutional knowledge, defined escalation rules, and ongoing automated quality monitoring.
| Point | Details |
|---|---|
| Two-layer architecture | Separate inquiry capture from human escalation to maintain clinical safety and accuracy. |
| RAG over base models | Retrieval-augmented generation grounds AI responses in your specific protocols, not general training data. |
| Accuracy is specialty-specific | The ~76% overall accuracy rate varies by domain; test in your clinical context before full deployment. |
| BAA is non-negotiable | Every AI vendor handling PHI must sign a Business Associate Agreement before any patient data is processed. |
| Automate your QA | Automated evaluation pipelines aligned with clinician ratings make ongoing oversight operationally realistic. |
The part most administrators get wrong
I have watched clinics make the same mistake repeatedly: they evaluate AI inquiry systems based on demo performance and vendor promises, then deploy without defining what “good enough” looks like in their specific clinical environment. The 76% accuracy figure from the Penn State research is not a benchmark to celebrate. It is a ceiling to work against.
Here is what I have found actually works. The clinics that get real operational value from AI inquiry handling are the ones that treat the AI like a new staff member on probation. They define the scope tightly, monitor performance weekly in the first 90 days, and expand the AI’s autonomy only after the data supports it. They do not hand the AI the full inquiry volume on day one and hope for the best.
The other thing worth saying plainly: the human escalation layer is not a fallback for when the AI fails. It is a designed feature of the system. The clinics that try to minimize escalation to reduce cost end up with patient safety exposure they cannot afford. The goal is not to eliminate human review. The goal is to make human review faster and better by giving clinicians structured, AI-prepared information instead of raw, unfiltered patient messages.
If you are planning an AI adoption in 2026, start with why medical practices need AI tools as a framework, then build your deployment plan around your specific inquiry volume, specialty, and compliance posture. The technology is ready. The question is whether your operational plan is.
— Adam
How Pulp AI Studio helps clinics automate patient inquiries
Pulp AI Studio builds AI-powered systems specifically for clinics that cannot afford to miss a patient inquiry, whether it arrives at 2 PM or 2 AM. The automated medical answering service handles inbound patient calls, routes inquiries by type, and captures after-hours requests before patients call a competitor. The missed call text-back system responds within 30 seconds of a missed call, keeping the patient engaged while your staff is unavailable. Deployment takes two weeks, and you own the rig. For clinics ready to stop losing patients to voicemail, Pulp AI Studio’s after-hours answering service is a fixed-cost solution that runs every hour your front desk does not.
FAQ
How does AI classify different types of clinic inquiries?
AI systems use intent classification models to sort patient messages into categories such as scheduling, billing, clinical questions, and urgent concerns. Each category triggers a different response path, with clinical and urgent inquiries routed to human staff.
What is the accuracy rate of AI for medical questions?
LLM responses to health queries achieve roughly 76.2% overall accuracy, with error rates exceeding 20% depending on medical specialty. This makes human escalation protocols a required component of any clinical AI deployment.
Does AI for patient inquiries require HIPAA compliance?
Yes. Any AI system that processes protected health information is classified as a HIPAA business associate, requiring a signed BAA and technical safeguards including encryption, access controls, and audit logging.
What is retrieval-augmented generation and why does it matter for clinics?
Retrieval-augmented generation (RAG) allows an AI system to pull from your clinic’s specific protocols and knowledge base before generating a response, rather than relying solely on general training data. This is what makes clinic-specific AI more accurate and safer than a generic chatbot.
How do clinics monitor AI inquiry quality at scale?
Automated evaluation pipelines that measure response completeness, evidence use, and medical accuracy can match clinician judgment without requiring manual expert review of every interaction. These pipelines make ongoing quality assurance operationally realistic for clinics of any size.