TL;DR:
- AI in healthcare redesigns workflows and reallocates clinician roles, creating a systemic shift rather than simple automation.
- Successful AI integration requires embedding tools into existing systems, proactive governance, and involving frontline staff early to ensure adoption and meaningful results.
Most clinic managers assume AI is about automation. It isn’t. The role of AI in clinic operations runs much deeper than replacing paperwork or triaging appointment requests. AI functions as a capacity multiplier, one that redesigns how work flows through your practice, who handles what, and where physicians actually spend their cognitive energy. You are not adding a tool to an existing system. You are restructuring the system itself. This article breaks down what that looks like in practice, where the real value comes from, and how to implement it without creating new chaos in the process.
Key takeaways
| Point | Details |
|---|---|
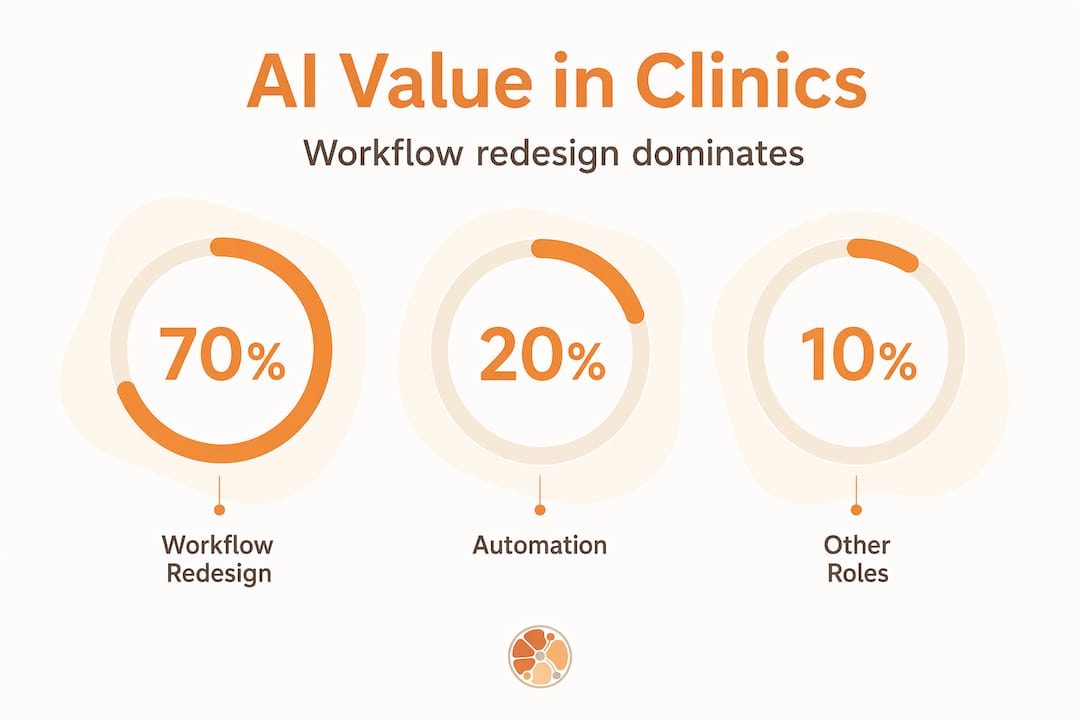
| AI redesigns workflows, not just tasks | About 70% of AI value in health care comes from workflow redesign and role redefinition, not model deployment alone. |
| Embed AI at the point of decision | Integrating AI directly into EMR and HIS systems drives faster adoption and measurable operational savings. |
| Governance is ongoing, not a one-time step | Continuous model monitoring, drift detection, and shared stakeholder oversight are non-negotiable for safe AI use. |
| Clinician involvement drives adoption | Frontline staff who participate in AI design and rollout report significantly better workflow fit and less resistance. |
| Post-launch iteration determines real ROI | Budgeting for feedback loops and real-world course correction after deployment is what separates successful implementations from abandoned ones. |
How AI transforms clinic workflows and human roles
Here is the way to think about it. AI does not just speed up your existing process. It reroutes it entirely. The biggest misconception in AI in healthcare management is that you deploy a model and watch efficiency numbers rise. What actually happens, when done right, is that AI takes ownership of the routine synthesis and coordination work across the entire patient journey, from intake to discharge to follow-up scheduling, and frees your clinical staff to handle exceptions, judgment calls, and complex care decisions.
BCG research shows that AI-first health providers generate roughly 70% of their value from workflow redesign and role redefinition, not from the AI models themselves. That is a number worth sitting with. You could have the most sophisticated AI model available and still see minimal operational gains if the workflows around it stay the same.
What does redesigned work look like in practice? Think of AI as the coordinator that never sleeps and never loses a record. It synthesizes labs, flags anomalies, routes prior authorization requests, and populates documentation fields while your clinicians review results and talk to patients. Humans focus on exceptions. AI handles the connective tissue.
The benefits of AI in clinic operations become visible when you stop measuring by task completion and start measuring by throughput and staff workload distribution. A well-deployed system does not just complete tasks faster. It shifts which tasks land on a physician’s desk at all.
- AI routes incoming patient data to the right care team member based on urgency and specialty
- Routine coordination, like appointment reminders, follow-up messages, and pre-visit questionnaires, runs without human input
- Documentation that once took 20 to 30 minutes per patient gets reduced to review and sign-off
- Administrative bottlenecks, such as referral tracking and eligibility checks, get resolved before staff even notice them
Pro Tip: Before selecting any AI tool, map your current patient journey end to end. Mark every touchpoint where staff are doing coordination work rather than clinical work. Those are your highest-value AI insertion points.
Successful deployments replace manual approvals with embedded automation plus human exception handling. That model scales. One-off automations do not.
Real-world examples of AI integration
The impact of AI on clinics is no longer theoretical. You can look at what institutions have already done and steal the playbook.

Cleveland Clinic is the clearest case study available right now. Within one year, they trained 5,000 providers on ambient listening AI, which automatically transcribes clinical conversations into structured notes. The result was a documented 40% reduction in unused operating room time. That is not a documentation improvement. That is a surgical throughput improvement triggered by removing a paperwork burden.
| AI application | Operational impact | Example |
|---|---|---|
| Ambient listening and transcription | Reduces documentation time per visit | Cleveland Clinic, 5,000+ providers trained |
| Revenue cycle automation | Accelerates claim processing and reduces denials | Automated eligibility checks and coding assistance |
| Virtual command centers | Improves OR scheduling and patient transfer coordination | Real-time bed management and transfer logistics |
| AI-enabled triage and routing | Reduces wait times and staff interruptions | Automated intake screening before a physician sees the patient |
IHH Healthcare took a different angle. By embedding AI directly into workflows, integrated within their existing clinical systems rather than as a standalone overlay, they saved up to 800,000 hours annually across their hospital network. That is the difference between AI that sits beside a workflow and AI that lives inside it.
Revenue cycle is another area where AI applications in medical practices are delivering measurable returns. AI-enabled prior authorization, automated coding suggestions, and denial prediction tools cut the lag between service delivery and payment processing significantly. For smaller clinics, that cash flow acceleration matters immediately.
- Ambient AI handles transcription, letting physicians stay present in the exam room
- Automated patient communication tools manage urgent text workflows without manual intervention
- Predictive scheduling reduces no-show rates by sending smarter reminders based on patient history
- Revenue cycle tools flag potential denials before claims are submitted
The common thread in every successful deployment is integration. AI tools that exist outside core clinical systems get abandoned. AI tools that live inside the systems clinicians already use get adopted.
Best practices for embedding AI into clinical workflows
Knowing AI works is not the same as knowing how to make it work inside your clinic. Here is a structured approach that holds up across different practice sizes and specialties.
-
Embed AI at the point of decision. Do not build a separate AI dashboard your staff has to remember to check. Integrate AI outputs directly into your EMR or HIS so alerts, suggestions, and documentation assistance appear inside the tools clinicians already use. The 800,000 hours saved at IHH Healthcare came from this exact approach.
-
Build governance before you need it. The Vector Institute’s 2026 roadmap treats AI governance as end-to-end lifecycle management, which includes model drift detection, ongoing validation, and regular performance reviews. Set this up before your first deployment, not after something goes wrong.
-
Assign shared oversight responsibilities. AI governance cannot live in one person’s job description. Create a cross-functional group that includes clinicians, administrators, and IT. Each group catches different failure modes.
-
Involve frontline staff early. Studies show that nurses and frontline staff report significantly better workflow fit when they participate in AI tool design and testing before launch. This is not just about morale. It is about catching workflow mismatches before they cost you adoption.
-
Budget for post-launch iteration. Most clinics underestimate this. The first 60 to 90 days after deployment will surface real-world edge cases that your vendor never anticipated. You need dedicated time and budget to address them.
-
Monitor continuously. Model drift, where an AI’s performance degrades as real-world data shifts away from training data, is a genuine operational risk. Build monitoring into your ongoing operations, not just your launch checklist.
Pro Tip: When evaluating AI vendors, ask specifically how they handle model updates and performance degradation over time. A vendor with no clear answer to that question is selling you a launch, not a solution.
How AI improves clinic efficiency at scale depends almost entirely on how well these practices get executed. The technology is ready. The operational discipline is what separates results from regret.
Common challenges and how to overcome them
AI adoption inside clinics is not a plug-and-play experience. The technology is only part of the equation.
The most common mistake is treating AI deployment as a technology project rather than an operational redesign. When that happens, you get a new tool bolted onto old workflows. Staff work around it. The ROI never materializes. Post-launch feedback loops and real-world course correction are what actually deliver value after go-live, according to KFF analysis of AI at scale in health care.
Regulatory compliance sets a floor, not a ceiling. FDA authorization alone does not make an AI tool safe for your specific clinical environment. Shared governance by your health system, clinicians, and operational leaders is what closes the gap.
A few practical strategies for navigating the real barriers:
- Avoid vendor lock-in by prioritizing AI tools that connect to your existing data infrastructure rather than creating a separate data silo
- Plan for data quality issues upfront. AI performance is only as good as the data it runs on, and most clinics discover gaps they did not know existed
- Address clinician skepticism directly. The question “what happens when the AI is wrong?” needs a clear documented answer before deployment
- Set expectations across the organization that the first version of any AI tool will require adjustment
The clinics that navigate these challenges successfully treat each obstacle as a data point, not a failure. That mindset matters more than the specific AI tool you choose.
Future trends in AI and healthcare operations
The trajectory is clear. AI applications in medical practices are moving from operational efficiency toward personalized, proactive care delivery.
- Generative AI is reducing documentation time by 15% per consultation among frequent users, with discharge summaries, referral letters, and care plans being auto-drafted for physician review
- AI tools are expanding beyond the back office into direct patient-facing functions, including personalized follow-up communication and chronic disease monitoring
- Physician AI adoption rates are accelerating as ambient tools prove their value in real clinical settings, reducing the cultural resistance that slowed early deployments
- Clinics that lack internal digital capability are forming strategic partnerships with specialized AI providers to fill gaps quickly rather than building from scratch
The clinics that get ahead in the next two years will not necessarily be the ones with the biggest budgets. They will be the ones that build organizational AI maturity now, with the right governance, the right integrations, and the right people involved at every stage.
My honest take on AI adoption in clinics
I’ve watched clinics spend six figures on AI tools and see almost no operational return. I’ve also seen smaller practices with modest budgets achieve genuinely significant results within a few months. The difference is never the technology. It’s always the approach.
What I’ve learned is that AI adoption is a cultural transformation that uses technology as its vehicle. When you deploy AI without redesigning the roles and workflows around it, you are essentially asking your staff to do their old jobs plus manage a new tool. That is not capacity multiplication. That is burden addition.
The clinics I find most inspiring are the ones that ask the uncomfortable questions before they buy anything. Questions like: Which decisions are we currently making that AI could handle better? Which bottlenecks exist because of coordination failure rather than clinical complexity? Those questions lead to AI deployments that stick.
I’ve also seen the trap of over-governance slow things down to the point of paralysis. You need oversight, but you also need movement. The answer is building lightweight governance structures early so you can move fast and still catch problems before they compound.
AI in healthcare management is not a destination. It is an operating discipline. The clinics treating it that way are already years ahead.
— Adam
How Pulp AI Studio helps clinics stop losing patients after hours
The biggest gap most clinics overlook isn’t inside their EMR. It’s what happens when a patient calls at 6 PM and no one picks up. That missed call becomes a lost patient before your front desk opens tomorrow morning.
Pulp AI Studio’s automated medical answering service handles exactly that gap. AI-powered auto-replies engage patients within 30 seconds of a missed call, keeping them connected before they turn to a competitor. The setup is live within two weeks as a scoped build you own. For clinics that want to reduce ghosting and increase patient retention without hiring additional staff, this is where you start.
FAQ
What is the role of AI in clinic operations?
AI in clinic operations functions as a workflow orchestrator, handling routine coordination, documentation, and communication tasks so clinical staff can focus on complex care and exceptions. The greatest value comes from redesigning workflows around AI, not just deploying tools on top of existing processes.
How does AI improve clinic efficiency?
AI improves efficiency by automating documentation through ambient listening, accelerating revenue cycle processing, reducing no-show rates through predictive scheduling, and managing patient communications without manual intervention. Clinics like IHH Healthcare have documented up to 800,000 hours saved annually through workflow-integrated AI.
What are the biggest challenges in adopting AI in a clinic?
The most common challenges are treating deployment as a technology project rather than an operational redesign, data quality issues, clinician resistance when staff aren’t involved early, and underestimating the budget needed for post-launch iteration and ongoing model monitoring.
Do clinics need FDA approval to use AI tools?
FDA authorization is required for certain clinical AI tools, but it sets a regulatory floor rather than a complete safety guarantee. Health systems must implement their own shared governance frameworks that include clinicians, administrators, and IT stakeholders to ensure safe and appropriate use in their specific environments.
How long does it take to see results from AI in a clinic?
Timelines vary by tool and deployment approach, but clinics with strong workflow integration and clinician involvement typically see measurable operational improvements within 60 to 90 days. Post-launch feedback loops and continuous monitoring are what convert initial gains into sustained results.